Breastfeeding in Mauritius: Everything You Need to Know and Everything Nobody Tells You
- Aurelie
- 21 mins read
I want to say something before we start.
Whatever you have been told about breastfeeding… that it comes naturally, that every Mauritius woman has always done it, that if you struggle it means something is wrong with you or your milk… I want you to set it aside for a moment.
Because here is the truth that this page is built on: breastfeeding is natural, but it is not automatic. It is a skill. One that you learn, that your baby learns, that the two of you figure out together in the exhausted, emotional, sometimes painful, sometimes extraordinarily beautiful days after birth. And like any skill worth having, it is far easier to learn when someone explains it properly rather than handing you a baby, wishing you luck, and closing the clinic door behind them.
In Mauritius, there is a commercial story about infant feeding that has been told loudly and consistently for decades. Formula companies have been present in our pharmacies, our clinics and our cultural imagination for so long that many families now assume formula is the default and breastfeeding is the exception. That a struggling mother should reach for a tin rather than for support.
Nutura exists, in part, to tell a different story.
Not because formula is evil. Not because every woman must breastfeed regardless of her circumstances or wishes. But because the women who want to breastfeed, who set out to breastfeed, deserve accurate information, genuine support, and the confidence that comes from understanding what is happening in their body and their baby’s. And right now, in Mauritius, that support is limited and somehow hard to find.
This page is that support.
Why breastfeeding matters: the evidence, plainly stated
The research on breastfeeding is not ambiguous. It is among the most consistent bodies of evidence in all of infant nutrition science, replicated across decades and across populations. The World Health Organisation recommends exclusive breastfeeding for the first six months of life, with continued breastfeeding alongside solid foods for two years or beyond. This is not a lifestyle recommendation. It is a public health position based on outcomes for babies and mothers.
For your baby, breast milk provides something no formula can replicate: a living fluid that changes composition in response to your baby’s age, her developmental stage, the temperature on a particular day, and even the specific pathogens she has been exposed to. The antibodies in your breast milk are produced by your immune system in direct response to what your baby is encountering. No manufacturing process can do this. It is your body, responding to your baby, in real time.
Beyond immunity, the research consistently links breastfeeding with reduced rates of respiratory infection, gastrointestinal illness, ear infections, and sudden infant death syndrome. Longer-term, breastfed babies show lower rates of obesity, type 2 diabetes, and certain childhood cancers. In Mauritius, where diabetes prevalence is among the highest in Africa and the Indian Ocean region, this is not an abstract statistic. It is a public health reality that starts with what we feed our babies.
For you, breastfeeding supports postpartum recovery in ways that matter for your body long after the newborn stage. Oxytocin released during feeding causes uterine contractions that reduce postpartum bleeding and help the uterus return to its pre-pregnancy size more quickly. Extended breastfeeding is associated with reduced risk of breast and ovarian cancer, reduced risk of type 2 diabetes, and lower rates of postpartum depression. The hormones of breastfeeding (prolactin and oxytocin) are the hormones of calm, of attachment, of the particular closeness between a mother and her baby in those early weeks.
And then there is the thing that no research paper fully captures: the feeling of your baby at your breast, settled and content and completely yours, in the quiet of a 3am feed when the rest of the world is asleep. That is yours. No one can give it to you and no one can take it away.
The Mauritius context: what we are working against together
Breastfeeding rates in Mauritius have declined significantly over the past three decades, tracking the pattern seen across much of the developing world as formula marketing expanded its reach into clinics, hospitals, and family culture.
Many Mauritius mothers are surrounded by voices, from family, from neighbours, from well-meaning clinic staff themselves, that introduce doubt about breast milk in the earliest days. Ti bébé la affamé. Baby is hungry. You do not have enough milk. He needs formula to grow properly. Your milk has not come in yet, just supplement with formula. I will never forget my second day at the clinic after birth because the pediatrician was so sure that my baby was not having enough milk (despite 5 wet diapers) and ordered a glucose test to make sure that she was not starving and dehydrated!
These messages often arrive in the first 48 to 72 hours after birth, precisely when breast milk has not yet come in and colostrum (the thick, golden, concentrated first milk) is the only thing being produced. Colostrum looks like very little. It is not very little. It is exactly what a newborn needs in exactly the amounts a newborn needs it. But without that knowledge, without someone explaining what colostrum is and why it is enough, the doubt wins.
The tin goes in. The feeding at the breast decreases because the baby’s hunger is being met elsewhere. Milk supply, which operates on a supply-and-demand system, does not build to its full capacity. And what started as a well-intentioned bottle in the hospital becomes the norm by the end of the first week.
This is not blame. It is a system that has failed mothers by removing information and replacing it with a commercial product. Nutura’s role is to return the information.
The complete breastfeeding guide: navigate by what you need
Getting started: the first hours matter more than anything
The most important thing you can do for breastfeeding success happens in the first hour after your baby is born.
Skin-to-skin contact (your naked baby placed directly on your bare chest) triggers a cascade of biological responses in both of you. Your baby’s temperature regulates against yours. Baby’s blood sugar stabilises, stress hormones drop, and baby’s rooting reflex (the instinct to turn her head, open her mouth, and search for the nipple) is at its most active and instinctive in the first hour of life. Babies placed skin-to-skin in this window often latch themselves with minimal intervention. This is not a metaphor for bonding. It is neurological programming, and using it is the single most powerful thing you can do in that first hour.
Ask for this explicitly at your Mauritius clinic or hospital before you give birth. Put it in your birth preferences. Say clearly: I want immediate skin-to-skin contact unless there is a medical reason this is not possible. Both immediately after a vaginal birth and after a C-section, your baby can be placed on your chest in theatre while you are being closed. Ask.
The latch (how your baby attaches to the breast) is the technical foundation of everything that follows. A correct latch is not painful beyond the first few seconds of initial discomfort in the early days. If feeding hurts throughout every feed, something about the latch needs to change. Pain is information, not endurance. The most common latch issue is a shallow latch where your baby taking only the nipple rather than a large mouthful of breast tissue including the areola. This causes nipple damage, reduces the efficiency of milk transfer, and signals to your body that less milk is needed than actually is.
Signs of a good latch: your baby’s mouth is wide open, taking in a large amount of breast tissue; her chin is touching your breast; her lower lip is flanged outward rather than tucked under; you can hear rhythmic swallowing after the initial rapid sucking; and feeding is uncomfortable for the first ten seconds then eases. If any of these are absent, break the seal with your clean finger inserted at the corner of the mouth, and try again.
Colostrum: the first milk your body makes
In the first two to four days after birth, your body produces colostrum rather than mature breast milk. Colostrum is thick, sticky, and present in very small amounts, typically 5 to 7ml per feed in the first 24 hours. This is not a failure of your supply. It is exactly what your baby’s stomach (currently the size of a marble) can hold.
Colostrum is sometimes called liquid gold, and the description is apt. It is extraordinarily concentrated in antibodies, particularly immunoglobulin A, which coats your baby’s gut lining and provides her first immune protection against the world outside the womb. It has a laxative effect that helps clear meconium (the dark first stool) from your baby’s digestive system and its small volume means your baby’s digestive system is not overwhelmed before it is ready.
Your milk will come in between days two and five. When it does, your breasts will become noticeably fuller, heavier, and possibly quite hard. This is engorgement, and it is normal, temporary, and manageable. Feed frequently. Apply a warm cloth before feeds to encourage letdown. Apply a cold cloth after feeds to reduce swelling. The engorgement eases within 24 to 48 hours as your body calibrates supply to demand.
Feeding patterns: what is actually normal
This is the section where the most well-intentioned misinformation lives.
A breastfed newborn feeds between 8 and 12 times in every 24 hours. That is every 1.5 to 3 hours, including at night. This is not a sign of insufficient supply. This is normal newborn feeding behaviour driven by the combination of a small stomach capacity, highly digestible breast milk that moves through the system quickly, and the demand-based supply system that requires frequent feeding in the early weeks to establish full milk production.
Cluster feeding: periods where your baby feeds almost continuously for several hours, typically in the early evening, is one of the most misread feeding behaviours in new parenting. It looks like your milk has run out. It looks like your baby is starving and your supply is inadequate. It is almost always neither of those things. Cluster feeding is your baby’s method of stimulating a supply increase ahead of a growth spurt, and it is a perfectly calibrated biological system. The evening cluster feed is also when your baby is building the fat stores and calories she needs for the longer stretch of sleep that will eventually come.
The formula bottle offered during a cluster feed is the single most common way breastfeeding ends earlier than a mother intended. Because it works — the baby fills up and stops fussing — and because the mechanism is not explained, so the mother concludes that what she observed (apparent starvation) was what was actually happening (supply increase in progress). Understanding cluster feeding is one of the most important things you can know before your baby arrives.
Growth spurts: at approximately 3 weeks, 6 weeks, 3 months, and 6 months, temporarily increase feeding frequency and can look like regression or supply problems. They last two to four days. The correct response is to feed more frequently, which communicates the increased demand to your supply system. Introducing supplementation during a growth spurt breaks the demand signal at precisely the moment your supply needs to respond to it.
Supply: how it works and what actually affects it
Breast milk supply is not fixed. It is responsive. Your body produces milk according to how much is being removed from the breast, and calibrates over the first six to eight weeks of breastfeeding to match your baby’s appetite precisely.
This means the most effective way to increase supply is to feed more frequently. Not to rest more. Not to eat specific foods first. Not to pump in addition to every feed from day one. Feed more. Empty the breast more completely at each feed. Signal to your body that more milk is needed.
Things that genuinely support supply: feeding on demand rather than to a schedule, ensuring effective transfer at each feed (which comes back to latch), adequate hydration, breastfeeding requires approximately 700ml of additional fluid daily above your normal intake in the Mauritius heat, and adequate overall nutrition without severe caloric restriction. Aim to at least 3L of fluids, ideally water, per 24h period.
Galactagogues: substances traditionally used to support milk production, include moringa (bred mouroum), fenugreek, fennel and oats. Moringa in particular has a long history of use across Mauritius and the Indian Ocean, and a growing evidence base supporting its use as a nutritional support for breastfeeding mothers. Our organic moringa infusion is available in the Nutura shop. It is not a medicine. It does not guarantee any specific outcome. What it provides is excellent nutritional support (iron, calcium, vitamin A, complete protein) at a stage when your nutritional demands are at their highest.
Things that genuinely reduce supply: introducing formula supplements without medical necessity (which reduces the demand signal), strict feeding schedules in the early weeks, extreme stress and chronic sleep deprivation (which suppress prolactin), smoking, and certain medications. Always check with your healthcare provider before taking any medication while breastfeeding, the resources at LactMed (lactmed.nlm.nih.gov) provide a searchable database of medications and their compatibility with breastfeeding.

Common challenges: and that they are solvable
Nipple pain is the most common reason women stop breastfeeding in the first two weeks. It is also, in the vast majority of cases, a latch problem with a latch solution. Cracked, bleeding nipples are not the price of breastfeeding, they are a sign that something needs to change about how your baby is attaching. A lactation consultant can assess and correct a latch in a single home visit. This is the most effective Rs 1,500 to Rs 2,500 you will spend in the postpartum period.
In the meantime: best remedy is to have a few breastmilk drops on your nipple and let nipples air dry after feeds where possible. Avoid using soap on the nipple area, it strips the natural oils that protect the skin.
Mastitis is an inflammation of breast tissue, hot, red, painful area in the breast, often accompanied by flu-like symptoms, fever, and chills. It is not necessarily caused by an infection, though it can become infected if untreated. The correct response to mastitis is to continue feeding or pumping from the affected breast. Stopping will only make it worse. Apply warmth before feeds, cold after. If symptoms have not improved within 24 hours, or if you develop a fever above 38.5°C, contact your doctor, antibiotics may be needed and are safe to continue while breastfeeding.
A mastitis that is not treated can progress to a breast abscess, which is significantly more serious. Do not push through mastitis hoping it will resolve without attention. It rarely does.
Low supply concerns: genuine low supply is less common than perceived. Most cases of apparent low supply are either: normal newborn feeding frequency misread as demand, a latch issue reducing transfer efficiency, or the aftermath of early supplementation that has reduced the demand signal. Before concluding that supply is truly low, consult a lactation consultant. The assessment of what is actually happening, versus what appears to be happening, changes the response entirely.
Actual indicators that your baby is getting sufficient milk: minimum six wet nappies per day from day five onwards, soft yellow stools in breastfed babies, your baby returning to birth weight by days ten to fourteen, and steady weight gain at subsequent checks.
Nutrition for breastfeeding mothers in Mauritius
You do not need a special diet to breastfeed. You need enough food. Breastfeeding requires approximately 500 additional calories per day above your pre-pregnancy intake, not a license to eat anything, but a clear instruction not to restrict severely while you are feeding a baby.
The foods that support both your health and your milk supply: dark green leafy vegetables including bred mouroum, protein at every meal (eggs, fish, lentils, legumes, meat), wholegrains (brown rice, oats), healthy fats (avocado, nuts, fish), and fresh fruit rich in vitamin C. The traditional Mauritius diet — dal, rice, fresh fish, vegetables, fruit — is excellent nutritional support for breastfeeding when eaten in adequate quantity.
Foods that some breastfed babies respond to with fussiness or wind: very spicy meals, large amounts of caffeine, and occasionally cruciferous vegetables (chou-fleur, chou). These reactions are individual and many breastfed babies are entirely unaffected by their mother’s diet. Do not eliminate food groups preemptively. If you notice a consistent pattern, a specific food followed by a specific reaction in your baby within 2 to 4 hours, try removing it for a week and observe. But do not restrict your diet based on fear rather than evidence.
Hydration is the nutritional intervention with the clearest supply impact. Keep a large water bottle at your feeding spot. Drink before you feel thirsty. In Mauritius heat, this requires more deliberate effort than in cooler climates.
Returning to work: 16 weeks is not enough, but it is what we have
Mauritius maternity leave is 16 weeks for one child and 18 weeks for twins (or more) and premature births. This means many mothers return to work when their baby is four months old, before solids have started, before sleep has consolidated, before the breastfeeding relationship has fully established its rhythm.
This is the reality of working motherhood in Mauritius, and nutura.org is not going to pretend it is anything other than what it is: a policy that makes breastfeeding significantly harder than it needs to be, for working women who want to continue.
What is possible: pumping at work. A good quality double electric pump (an investment worth making) allows you to maintain your supply during working hours by expressing milk every three hours, approximately. Your employer is legally required to provide nursing breaks under Mauritius employment law. Know your rights before you return.
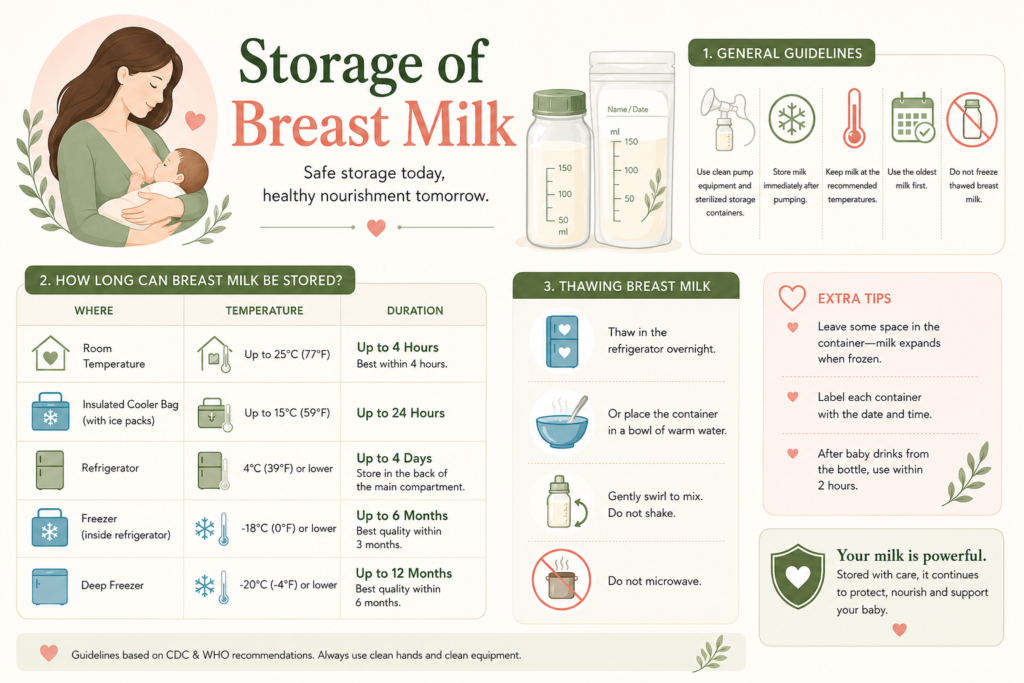
The practical logistics: a small cool bag with ice packs keeps expressed milk safe for transport. Breast milk can be stored in the refrigerator for up to five days and in a freezer for up to three months. Label every bag with the date. Build a small freezer stash in the weeks before returning to work — one extra pump session per day, the milk stored and labelled, reduces the pressure of that first week back considerably.
The ebook coming to nutura.org
Everything above is the beginning of what you need to know. The complete breastfeeding guide — coming soon to nutura.org — goes further into every dimension of this: the day-one success plan, feeding patterns week by week, the full nutrition guide with a 7-day meal plan, supply management in depth, partner and family support (how to involve the people around you and how to set limits on the advice that undermines you), and a 7-day action plan with a printable breastfeeding checklist for the first week home.
If you want to be notified the moment it is available, subscribe to the Nutura newsletter below.
Quick answers — the questions every breastfeeding mum asks
How do I know my baby is getting enough milk?
Six or more wet nappies per day from D5. Soft yellow stools. Birth weight regained by day ten to fourteen. Steady weight gain at checks. A baby who feeds, settles, and has periods of content wakefulness. These are your indicators, not the volume in a bottle, which is the only metric bottle feeding provides and which breastfeeding does not.
When should I start pumping?
If breastfeeding is established and going well, there is no rush to introduce a pump in the first weeks. The exception: if you are separated from your baby for any reason, or if your baby cannot feed directly at the breast. If you plan to return to work at 16 weeks, begin building a small freezer stash from around week 6 to 8 with only one extra pump session daily, preferably in the morning when supply is naturally highest.
Can I breastfeed in public in Mauritius?
Legally and ethically, yes. Practically, Mauritius is a conservative culture in some spaces and you may encounter reactions that are not supportive. A good nursing cover or a loose outer layer gives you discretion if you want it. Many Mauritius mums have breastfed in shopping centres, restaurants, and family gatherings without incident. You are feeding your baby. That is never something to apologise for.
Can I mix breastfeeding and formula?
Yes, combination feeding is an option, and there are situations where it is the right choice for a family. What to understand before introducing formula: each formula feed that replaces a breastfeed reduces the signal to your supply by exactly that amount. Occasional supplementation may not affect supply significantly. Regular supplementation across multiple feeds per day will reduce supply over time. If you are considering combination feeding, discuss the timing and frequency with a lactation consultant so you can make the choice with full information about the supply implications.
What if breastfeeding is not working despite trying everything?
Some women are genuinely unable to breastfeed due to insufficient glandular tissue, previous breast surgery, certain medical conditions, or circumstances that make it impossible despite every effort. This is real, and it deserves acknowledgement rather than guilt. Breast milk from a donor milk bank, if available, is the next-best option. Formula is a safe, nutritionally adequate feeding choice when breastfeeding is genuinely not possible. Nutura’s position is not that formula is wrong. It is that formula should be a considered, informed choice, not a default reached for at the first moment of difficulty, before support has been given a chance to work.
The one thing this page wants you to know
Breastfeeding is the oldest, most tested, most nutritionally sophisticated form of infant feeding that has ever existed. It has sustained human babies for the entirety of human history, including in conditions far more difficult than a Mauritius summer.
The reason it sometimes fails in the modern context is not because it stopped working. It is because the support structures around it (the knowledgeable older women, the experienced midwives, the community of breastfeeding mothers) have been eroded, often deliberately, by commercial interests that profit from that erosion.
You can choose to breastfeed with full knowledge of what it involves, full access to support when you need it, and full permission to ask for help rather than reach for the tin.
That is what nutura.org is here for.
~ From a Mama, 12 months pp and still breastfeeding
Related Articles on Breastfeeding:
References: World Health Organisation — Breastfeeding. who.int/nutrition/topics/exclusive_breastfeeding. UNICEF UK — Breastfeeding in the UK. unicef.org.uk/babyfriendly. Victora C.G. et al. — Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. The Lancet (2016). Nambiar V.S. et al. — Moringa oleifera and lactation support: nutritional basis. LactMed — NIH database of drugs and lactation. lactmed.nlm.nih.gov. Mauritius Employment Rights Act 2008 — nursing break provisions.
Disclaimer: This page is for informational purposes only. It does not constitute medical advice. For personalised support with breastfeeding challenges, contact a qualified lactation consultant. In Mauritius, your clinic’s maternity department or a private LC in our directory is your first port of call.