Trying to Conceive in Mauritius: Your Honest, Complete TTC Guide
Understand your cycle, track ovulation, improve your fertility awareness, and navigate your trying-to-conceive journey with clarity and confidence.
You have made a decision. You are trying for a baby.
Maybe you came off contraception last month and you are already tracking everything. Maybe you have been trying for a while and the monthly hope-then-disappointment cycle is starting to take its toll. Maybe you are newly married and not yet sure when you will start, but you want to understand what trying to conceive actually involves before you get there.
Wherever you are in this, welcome. You are in the right place.
Trying to conceive (short term TTC) is one of the least talked about stages of the motherhood journey in Mauritius. There is no TTC clinic as such at your local health centre. Your gynaecologist will often only see you once you are already pregnant. Cultural expectations mean many women feel they should simply stop contraception and wait, without knowing that there are real, evidence-based things they can do to prepare their bodies, understand their cycles, and increase their chances of a healthy conception.
This guide covers all of it. Honestly. Without false promises, without overwhelming you, and without pretending that trying to conceive is simple or quick for every woman because for some it is not, and you deserve a resource that acknowledges that.
Explore Your TTC Journey
Menstrual Cycle
and understanding your Fertile Window
Nutrition
What you eat in the months before conception matters
Lifestyle
What Actually Matters and What Is Overstated
Tracking
Finding Your Fertile Window
When to See a Doctor
and what to ask
Partner’s Role
Male Fertility Matters Too
Emotional Reality of TTC
and How to Protect Yourself
From TTC to Pregnancy
What Happens Next
Understanding Your Menstrual Cycle and Your Fertile Window
Most women know roughly how their cycle works. Far fewer know the precise mechanics that determine when conception is possible and when it is not. Understanding this is the single most useful thing you can do when trying to conceive.
Here is the essential biology, without the textbook language.

Your fertile window: it is shorter than you think
The egg survives for only 12 to 24 hours after ovulation. But sperm can survive in the female reproductive tract for up to 5 days. This means your fertile window, i.e. the days when unprotected sex can result in pregnancy, is approximately 5 to 6 days: the 5 days before ovulation, and the day of ovulation itself.
The highest probability of conception comes from sex in the 2 days before ovulation and on the day of ovulation. Sex on the day after ovulation is largely too late.
For a typical 28-day cycle, this window falls roughly around days 10 to 15. But (this is critical) not all cycles are 28 days, and not all cycles are regular. Ovulation does not always happen on day 14. It can shift based on stress, illness, travel, weight changes, and a hundred other factors. This is why tracking matters.
What if your cycles are irregular?
Irregular cycles — those that vary significantly in length from month to month — can make identifying ovulation much harder. Common causes include polycystic ovary syndrome (PCOS), thyroid conditions, very low body weight, high stress, and perimenopause. If your cycles are consistently irregular, speak to your gynaecologist before spending months trying to identify your fertile window on your own. This is treatable, and a diagnosis changes what you should be doing.
Nutrition and Supplementation Before Pregnancy
What you eat in the months before conception matters, not just for your fertility, but for the very early development of a baby, which begins before many women know they are pregnant. The neural tube, which becomes your baby’s brain and spine, closes in the first 28 days after conception, often before your first appointment with you OB-GYN.
Pre-conception nutrition is not about a special diet. It is about building the best possible foundations before you need them.
Folic acid: the one supplement that is non-negotiable
Folic acid (vitamin B9) is the most evidence-supported supplement in pre-conception care. It significantly reduces the risk of neural tube defects — serious birth conditions affecting the brain and spine — and its protective effect works only when it is present in your body before conception, not after.
- Recommended dose: 400 micrograms (mcg) daily for all women trying to conceive. Start at least one month before you stop contraception — ideally three months before. Talking from experience here.
- Higher dose (5mg daily) if you: have previously had a pregnancy affected by a neural tube defect, have diabetes, are taking anti-epileptic medication, or have a BMI over 30. Discuss with your doctor.
- Available without prescription at all Mauritius pharmacies. Sold as standalone folic acid tablets or as part of a prenatal multivitamin.
Folate-rich foods (dark leafy vegetables, lentils, chickpeas, fortified cereals) help but are not a substitute for the supplement as cooking may reduce the folate content significantly.
Key nutrients for pre-conception
Nutrients and Why it Matters
- Iron: supports blood production; deficiency impairs fertility. Found in red meat, lentils, spinach, bred mouroum (moringa). Take with vitamin C to improve absorption. Mauritius has high rates of iron-deficiency anaemia — get your levels checked.
- Vitamin D: low levels linked to reduced fertility in both men and women. Mauritius sunshine is an advantage, but sun avoidance (for skin protection) and indoor work mean many Mauritius women are deficient. Ask your doctor to test your levels.
- Omega-3 fatty acids: support egg quality and hormonal balance. Mauritius fish (especially mackerel, sardines, tuna in moderation) is an excellent source. Avoid high-mercury species: swordfish, marlin, shark.
- Zinc: essential for egg maturation and healthy ovulation. Found in meat, shellfish, lentils, pumpkin seeds.
- B vitamins (particularly B12 and B6): support hormonal balance and reduce homocysteine, elevated levels of which are linked to fertility challenges. Found in meat, eggs, dairy, and fortified foods.
What to limit or avoid when TTC
- Alcohol: there is no established safe level during preconception or pregnancy. The safest approach is to stop completely when actively trying to conceive.
- High-mercury fish: swordfish, marlin, and shark are caught and sold in Mauritius but bioaccumulate mercury, which affects developing nervous systems. Avoid.
- Excessive caffeine: limit to 200mg per day (roughly one filter coffee or two cups of tea). High caffeine intake is associated with reduced fertility.
- Ultra-processed foods: diets high in processed food, refined sugar, and trans fats are associated with poorer fertility outcomes in both men and women.
- Unfermented soy in very large quantities: some research suggests very high soy intake may affect hormone levels. Moderate amounts (tofu, edamame) are fine.
- Certain herbal teas and supplements: not all are safe when TTC. Check with your doctor before taking anything beyond standard folic acid.
Moringa (bred mouroum) when trying to conceive
Moringa oleifera — the most nutrient-dense plant widely available in Mauritius — is an excellent nutritional foundation during the pre-conception period. Rich in iron, calcium, vitamin A, vitamin C, and protein, it supports the nutritional foundations that matter most before pregnancy.
In culinary quantities (as eaten traditionally in Mauritius cooking), moringa is safe and beneficial when trying to conceive. Highly concentrated supplements or extracts are a different matter — the evidence base is less clear, and very high doses may have hormonal effects. Use moringa as food, not as a concentrated supplement, during the TTC period.

Lifestyle Factors: What Actually Matters and What Is Overstated
The internet will tell you that you need to overhaul your entire lifestyle to conceive. Some of that advice is evidence-based. Some of it is wellness industry noise. Here is a clear-eyed breakdown of what the research actually shows.
What genuinely matters
High impact — act on these
- Healthy body weight: both underweight and overweight status can affect ovulation and fertility. This is not about appearance, it is physiology. Speak to your doctor about your individual situation rather than chasing an arbitrary BMI number.
- Stopping smoking: smoking significantly reduces fertility in both men and women, accelerates egg loss, and dramatically increases miscarriage risk. It is the single most impactful lifestyle change you can make.
- Stopping alcohol: particularly in the two weeks after ovulation (when implantation may be occurring), alcohol may interfere with early pregnancy establishment.
- Managing chronic conditions: uncontrolled thyroid conditions, PCOS, diabetes, and autoimmune conditions all affect fertility. Getting these managed before trying to conceive makes a measurable difference.
Lower impact — do not obsess
- Specific foods and ‘fertility diets’: no single food will make or break your fertility. A generally nutritious diet matters far more than any specific superfood or fertility recipe.
- Exercise: moderate regular exercise is beneficial for fertility. Extreme high-intensity training can disrupt ovulation in some women. For most people, continuing their current exercise routine is appropriate.
- Stress: while chronic severe stress can disrupt hormonal rhythms, the idea that ‘just relaxing’ will help you get pregnant is both scientifically oversimplified and deeply unhelpful to women who have been trying for months. Stress management matters for your wellbeing, not as a fertility fix.
- Underwear type (for partners): the evidence is inconsistent. Switching to boxers is low effort and risk-free, but it is not the solution if there is a significant issue.
A note on BMI and fertility in Mauritius
Mauritius has one of the highest rates of obesity and type 2 diabetes in Africa and the Indian Ocean region. Both conditions affect fertility but the relationship is complex, and the advice to ‘just lose weight’ is rarely helpful without support. If your doctor raises weight as a factor in your fertility, ask for a referral to a dietitian rather than trying to manage this alone. Crash dieting before pregnancy can deplete the very nutritional stores that matter most.
Tracking Your Cycle: Finding Your Fertile Window
Understanding when you are ovulating is the foundation of efficient TTC. There are several methods available, some high-tech, some low-tech, and all of them useful in different situations. Here is how they work and which might suit you best.
Method 1: Calendar tracking (basal method)
If your cycles are regular, you can estimate your ovulation by subtracting 14 days from the expected start of your next period. If your cycle is 30 days long, ovulation is likely around day 16. If it is 26 days, around day 12.
This is the simplest method but also the least reliable for women with irregular cycles. It works as a rough guide alongside other methods but should not be used alone.
Method 2: Basal body temperature (BBT) charting
Your resting body temperature rises by approximately 0.2–0.5°C after ovulation, due to the progesterone released by the corpus luteum. By tracking this temperature every morning before getting up — using a basal thermometer, which is more sensitive than a standard one — you build a picture of your cycle over several months.
- Take your temperature at the same time every morning, before any movement, after at least 3 hours of sleep.
- Record the reading in a dedicated app (Kindara, Fertility Friend, or a simple spreadsheet) to see the pattern emerge.
- BBT charting tells you that you have ovulated after the fact — the temperature rise confirms ovulation has occurred. It is most useful for understanding your pattern over several months, not for pinpointing the fertile window in real time.
- Accuracy is affected by illness, alcohol, disturbed sleep, travel, and stress — all of which can cause anomalous readings.
Method 3: Ovulation predictor kits (OPKs)
Ovulation predictor kits detect the surge of luteinising hormone (LH) that precedes ovulation by approximately 24–36 hours. A positive OPK tells you that your LH has surged and ovulation is imminent.
- Available at Mauritius pharmacies and online. Strip-based OPKs (less expensive) and digital OPKs (easier to interpret) are both effective.
- Test from approximately day 10 of your cycle (earlier for shorter cycles), once or twice daily.
- A positive result means ovulation is likely in the next 24–36 hours — this is your cue to have sex in the next 1–2 days.
- Women with PCOS may have persistently elevated LH, which can cause false positives with standard OPKs. Advanced digital monitors that measure both LH and oestrogen may be more useful.
Method 4: Cervical mucus observation
Your cervical mucus changes predictably throughout your cycle in response to oestrogen and progesterone. Learning to observe and interpret these changes — called the Billings Method or Creighton Model — gives you a real-time indicator of your fertility status.
- After your period ends: dry or minimal discharge.
- As oestrogen rises toward ovulation: mucus increases and becomes creamy, white, and opaque.
- At peak fertility: mucus is clear, slippery, and stretchy — often described as resembling raw egg white. This is your most fertile mucus. Ovulation typically occurs on the last day of this type of mucus or the day after.
- After ovulation: mucus becomes thick, sticky, and opaque again as progesterone rises.
Cervical mucus observation takes practice and a few cycles to understand your personal pattern. It is free, requires no equipment, and (once learned) is one of the most accurate natural fertility awareness methods available.
Combining methods gives the best picture
No single method is perfect for every woman. Many fertility specialists recommend combining OPKs (for real-time ovulation prediction) with BBT charting (for cycle pattern awareness) and cervical mucus observation (for additional confirmation). Together, these three methods give a comprehensive picture of your fertility across the month.
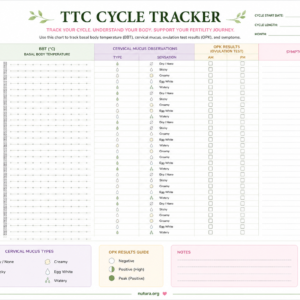
Download our free TTC cycle tracker
A printable cycle tracking chart designed for Mauritius women with columns for BBT, cervical mucus observations, OPK results, and symptoms. Free download.
Your Partner’s Role: Male Fertility Matters Too
In approximately 40-50% of couples experiencing fertility challenges, a male factor is involved, either as the primary cause or as a contributing one. This is not a reflection on masculinity. It is biology. And it is something that can often be addressed once identified.
In Mauritius, male fertility is significantly underdiagnosed, in part because cultural expectations around masculinity make it difficult for men to engage with this conversation. If you have been trying to conceive for more than 6 months without success, a semen analysis for your partner should happen at the same time as your own investigations, not as an afterthought.
What affects male fertility
Factors that reduce sperm quality
- Smoking: directly damages sperm DNA and reduces sperm count and motility
- Excessive alcohol consumption
- Anabolic steroids and testosterone supplementation: can cause temporary or permanent infertility
- Tight underwear and excessive heat to the scrotum (hot baths, laptop on lap, cycling for very long periods)
- Obesity: associated with lower testosterone and reduced sperm quality
- Certain medications: discuss with your doctor any regular medication your partner takes
- Previous STIs, particularly chlamydia and gonorrhoea, if untreated
- Varicocele: enlarged veins in the scrotum, which raises testicular temperature
What your partner can do now
- Stop smoking and reduce alcohol
- Take a supplement containing zinc, selenium, vitamin C, and vitamin E — all support sperm quality
- Maintain a healthy weight
- Manage any chronic conditions with their doctor
- Avoid hot baths and saunas during active TTC periods
- Get a semen analysis — this is a simple, non-invasive test available at private labs in Mauritius that gives you real information rather than guesswork
- See a urologist if there are any anatomical concerns or a history of testicular injury, mumps, or STIs
A note for partners reading this
If your partner has shared this guide with you, she is asking for something specific: your active participation in this process. TTC can be isolating for women as they carry most of the physical and emotional weight of tracking, timing, and waiting. Your engagement like taking your own health seriously, attending appointments together when possible, and being present for the emotional reality of this stage, makes a real difference. Thank you for reading.
When to See a Doctor and What to Ask
One of the most frustrating aspects of trying to conceive is not knowing when it is time to stop waiting and start seeking answers. Here is the guidance used internationally — and adapted for the Mauritius healthcare context.
When to seek a fertility review

Seek a review sooner than the timeline above if any of the following apply:
You have irregular or absent periods | You have been diagnosed with PCOS, endometriosis, or a thyroid condition | You have had pelvic inflammatory disease or a known STI history | Your partner has a known sperm issue | You have had more than one miscarriage | You have had previous abdominal or pelvic surgery | Something simply feels wrong — your instinct is a valid reason to seek answers
Where to go in Mauritius
- Public sector: area health centres offer basic reproductive health consultations. Referral to Victoria Hospital or Dr A.G. Jeetoo Hospital for further investigations if indicated.
- Private sector: your gynaecologist is the first port of call for fertility concerns. They can order the initial blood panel and semen analysis, and refer to a fertility specialist or reproductive endocrinologist if needed.
- Fertility clinics: there are private fertility clinics and specialists operating in Mauritius offering investigations and assisted conception. Ask your gynaecologist for a referral.
- Blood tests your doctor should order at a fertility review: day 2–3 FSH and LH (ovarian reserve markers), AMH (anti-Müllerian hormone — a stronger ovarian reserve indicator), prolactin, thyroid function, fasting glucose and insulin (particularly if PCOS is suspected), vitamin D, and a full blood count including iron studies.
- Scans: a pelvic ultrasound to assess the uterus and ovaries (including antral follicle count) is standard at a first fertility review and can identify PCOS, fibroids, and other structural factors.
The Emotional Reality of TTC: and How to Protect Yourself
Nobody talks about how hard trying to conceive can be. Not the physical tracking and timing — though that is exhausting enough — but the emotional cycle that accompanies it.
The hope that builds across the first half of your cycle. The hyperawareness of every possible symptom in the two-week wait. The crash of a period arriving. Then beginning again. Month after month after month. In Mauritius, where families are close and questions about when you are ‘starting a family’ are asked openly and repeatedly, this experience can feel particularly exposed.
You are allowed to find this hard. It is hard. And acknowledging that is not pessimism — it is honesty.
Protecting your mental health during TTC
- Set limits on how much time you spend on TTC forums and social media groups. They can be supportive, but they can also create unhelpful comparison spirals, amplify anxiety, and expose you to misinformation. Use them intentionally, not compulsively.
- Tell one trusted person in your life what you are going through — not necessarily your whole family, but someone who can hold this with you without pressure or unsolicited advice.
- Acknowledge the two-week wait for what it is: an emotionally difficult period of uncertainty that no amount of symptom-spotting will change. Distract yourself deliberately. Plan something you enjoy for the days before your period is due.
- Decide in advance how you will respond to ‘when are you having children’ questions from family and friends. Having a scripted, boundary-setting answer ready — ‘We are working on it’ or ‘We will let you know when there is news’ — reduces the emotional ambush of those conversations.
- Give yourself permission to take a break from TTC if you need it. A month without tracking, without timing, without apps can restore perspective and reduce the all-consuming nature of the process. Fertility does not stop while you rest.
Consider speaking to a counsellor or therapist if TTC is significantly affecting your mental health, your relationship, or your daily functioning.
If you have experienced a miscarriage or pregnancy loss
Pregnancy loss is devastatingly common — affecting approximately 1 in 4 pregnancies — and profoundly underacknowledged in Mauritius. If you are TTC after a loss, your grief and your fear are valid. You do not need to pretend this is simple. Allow yourself to grieve properly before beginning again. Speak to your doctor about investigations if you have had two or more losses. And please know — you are not alone in this, even when it feels that way.


From TTC to Pregnancy: What Happens Next
The day you see two lines on the test is one of the most significant moments of your life. Here is what to do in the hours and days that follow — so that when it happens, you know exactly where to go.
Immediately after a positive test
- Take a breath. You do not need to do anything urgently, unless you are experiencing one-sided pain or heavy bleeding, which can indicate an ectopic pregnancy and needs immediate medical attention.
- Stop alcohol, smoking, and any over-the-counter medications not cleared for pregnancy. If you are on prescribed medication, call your doctor before stopping anything abruptly.
- Start folic acid if you have not already (400mcg daily). If you were already taking it, continue.
- Book a first appointment with your gynaecologist or GP. In the public sector, your nearest area health centre is the starting point. In the private sector, call your gynaecologist directly.
- Do not go to hospital/ clinic unless you have pain, heavy bleeding, or a strong instinct something is wrong.
- Give yourself time to absorb what has just happened before telling people — you do not have to share immediately.
You are now in the pregnancy stage. Congratulations!
Your TTC journey has led you here. Everything you need for the first trimester and beyond is in our pregnancy section — written for Mauritius, from your first scan to your birth plan.
Grossesse
Week by Week, Symptoms & What to Expect

Bien-être maman
Postpartum, santé mentale et récupération : prenez soin de vous aussi.
FAQ GROSSESSE
How long does it normally take to get pregnant?
For couples having regular unprotected sex, approximately 84% will conceive within 12 months and 92% within 24 months. But averages mask huge individual variation. Some couples conceive in the first cycle; others take longer with no identifiable cause. Age is the most significant factor — fertility declines gradually from the mid-30s and more steeply after 37. If you are under 35 and have been trying for less than 12 months, you are within the normal range. If you are over 35 and have been trying for 6 months, it is time to seek a review. The statistics are informative but they are not your story — every situation is individual.
Can I get pregnant while breastfeeding?
Yes! this is a common misconception in Mauritius and globally. Breastfeeding suppresses ovulation in many women — particularly in the early months of exclusive breastfeeding — but it is not a reliable form of contraception. Ovulation can return before your first period does, meaning you can conceive without ever having had a postpartum period. If you are not ready to become pregnant again while breastfeeding, use contraception. If you are trying to conceive while breastfeeding, know that it is possible, though it may take longer for your cycle to become regular enough to time accurately.
Is it normal to stop having periods after coming off the pill?
Yes, and it is common. After stopping hormonal contraception, it can take 1 to 3 months for your natural cycle to reassert itself. Some women experience what is called post-pill amenorrhoea — absent periods for longer than 3 months. If your periods have not returned after 3 months off the pill, see your gynaecologist. This is usually a temporary hormonal adjustment rather than a sign of infertility but it should be investigated rather than waited out indefinitely, particularly if you are actively trying to conceive.
I have PCOS. Can I still get pregnant naturally?
Yes — most women with PCOS do conceive, though it often takes longer and may require support. PCOS affects ovulation, making it irregular or absent in some cycles, which is the primary fertility challenge. The good news is that PCOS is one of the most treatable fertility conditions. Lifestyle changes (particularly weight management if applicable, and reducing refined carbohydrates and sugar) can significantly improve ovulation in PCOS. Medication to induce ovulation — most commonly clomiphene citrate (Clomid) — is widely used and effective. Metformin is sometimes prescribed alongside. If you have PCOS and are trying to conceive, see your gynaecologist early rather than waiting the standard 12-month guideline.
We have been trying for 8 months. Should I be worried?
At 8 months, you are approaching the point where a fertility review is reasonable — particularly if you have any of the risk factors listed above in this guide (irregular cycles, PCOS, endometriosis history, previous STIs, age over 35). If you have none of these factors and are under 35, you have a few months within the ‘wait and try’ window remaining. However, there is no rule that says you must wait the full 12 months before asking for help. If you are anxious, if something feels wrong, or if you simply want the reassurance of knowing everything looks normal, book an appointment with your gynaecologist. A basic fertility panel — blood tests and a pelvic ultrasound — is non-invasive and gives you real information.
Is it safe to take prenatal vitamins before I am pregnant?
Yes — in fact, this is exactly what they are designed for. Prenatal vitamins are formulated to provide the nutritional support needed in the pre-conception period and the early weeks of pregnancy, when the neural tube is forming before most women know they are pregnant. Look for a prenatal multivitamin containing at least 400mcg folic acid, iron, vitamin D, iodine, and B12. Available at all Mauritius pharmacies. The only caveat: check with your doctor if you are on any other medication, as some nutrients interact with specific drugs.
Do I need to tell my employer I am trying to get pregnant?
No — you have no legal or professional obligation to disclose this. Mauritius employment law protects pregnant employees once pregnancy is established, but the TTC stage is entirely private. You may want to avoid heavy exposure to chemicals, X-rays, or other occupational hazards during the TTC period — speak to your doctor about your specific work environment if this is a concern. Beyond that, your family planning decisions are your own.
We have had one miscarriage. Do we need to be investigated before trying again?
One miscarriage is devastating, but it does not usually indicate a recurrent problem. Approximately 1 in 4 recognised pregnancies ends in miscarriage, and the majority are due to random chromosomal errors in the developing embryo — not to anything you did or a problem with either partner’s fertility. Most doctors will not investigate until a third consecutive miscarriage, as two miscarriages may still be within the statistical norm. However, if you have experienced two or more losses, ask for a recurrent miscarriage investigation — this includes blood tests for clotting disorders, chromosome analysis of both partners, and pelvic investigation. The emotional impact of miscarriage is significant, and you do not need to rush back into trying if you are not ready.
A word from us
TTC is one of the most private, hopeful, and sometimes heartbreaking chapters of a woman’s life. Whatever stage of this you are in right now — just starting, deep in the middle, or wondering if it will ever happen — you deserve information that treats you as an intelligent adult navigating something real. Not platitudes, not false promises, not advice that ignores what life is actually like on this island.
That is what Nutura is here to provide. We are glad you found us — and we will be here every step of the way, from this page all the way to your child’s first day of school.
— The team at Nutura | nutura.org
References & further reading
All content is reviewed for accuracy and updated regularly. Key references for this page:
- NICE Clinical Guideline CG156 — Fertility: Assessment and treatment for people with fertility problems. nice.org.uk (2013, updated 2017)
- World Health Organization — Selected practice recommendations for contraceptive use (WHO/RHR). who.int
- Folic Acid supplementation and neural tube defects: MRC Vitamin Study Research Group. Lancet (1991) — landmark RCT establishing the evidence base for folic acid supplementation.
- Gaskins A.J. et al. — Diet and fertility: a review. American Journal of Obstetrics and Gynecology (2018)
- Sharma R. et al. — Lifestyle factors and reproductive health: taking control of your fertility. Reproductive Biology and Endocrinology (2013)
- Miscarriage Association UK — Information on recurrent miscarriage and single pregnancy loss. miscarriageassociation.org.uk
- Billings Ovulation Method Association — Cervical mucus observation methodology. woomb.org
- Raspberry leaf tea and pregnancy: Holst L. et al. — Raspberry leaf — should it be recommended to pregnant women? Complementary Therapies in Clinical Practice (2009)
- Ministry of Health and Wellness Mauritius — Reproductive Health Programme. health.govmu.org
- Mauritius Non-Communicable Disease Survey 2015 — diabetes and obesity prevalence data. mohw.govmu.org
Disclaimer: All content on nutura.org is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional — gynaecologist, GP, or fertility specialist — for advice specific to your situation. In Mauritius, your nearest area health centre or private gynaecologist is your first point of contact for fertility concerns.